5. Religious group differences in deaths involving COVID-19, adjusted for socio-demographic factors
Differences in the risk of dying from the coronavirus (COVID-19) across different religious groups are dependent on factors related to the risk of being infected and the risk of dying given infection.
We use Cox proportional hazards regression models to estimate the risk of dying from COVID-19 across religious groups compared with the Christian population. The Christian population is used as the reference group because it has the largest population in the data used. We adjust the model for geographic, demographic, socio-economic, occupational exposure and self-assessed health measures from the 2011 Census; these characteristics have the potential to confound any association between COVID-19 mortality risk and religion. We therefore adjust for these in the model to estimate any excess risk for different religion groups. However, we are currently unable to adjust for factors such as prevalence levels of pre-existing conditions in religious groups; any unexplained increase in risk may be because of factors we have not accounted for as opposed to religion. The statistical models are explained in the technical appendix.
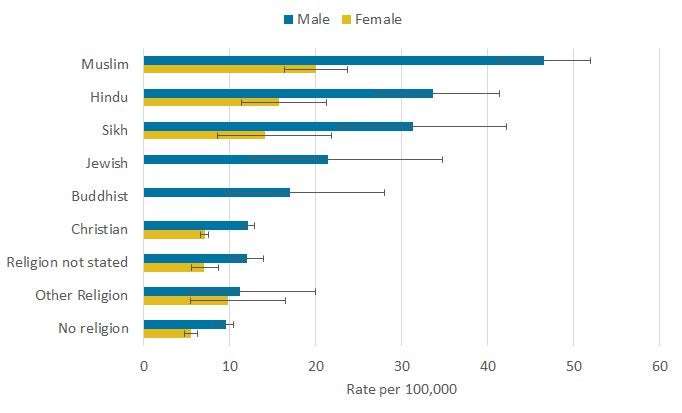
In Figure 3, we show how the risk of death involving COVID-19 varies by religious group for males and females. We report the hazard ratios relative to the Christian group (the reference group) for a range of geographic, demographic and socio-economic characteristics in green as well as for these plus a White and non-White ethnicity indicator (a marker of ethnicity) in blue. The hazard ratios in this analysis relate to the relative differences in the rate of deaths involving COVID-19, assuming survival until that point, between religious groups compared with the Christian group. A hazard ratio greater than one denotes that the outcome occurs at a greater rate than the reference group, while less than one indicates a lower rate.
The risk of death involving COVID-19 is highly correlated with age. After adjusting for age (in green), males and females from the Muslim, Jewish, Hindu and Sikh religious groups are at greater risk of a death involving COVID-19 compared with those identifying as Christian. Among Muslim males, the rate was 2.5 times greater than that for Christian males, while for females it was 1.9 times greater.
We also adjust for population density, region, rural and urban classification, area deprivation, household composition, socio-economic position, highest qualification held, household tenure, household exposure, and self-reported health and disability in 2011 (in blue). The fully adjusted results show differences in risk between religious groups that are specific to those religious groups and are unlikely to be associated with any of the factors listed earlier.
Figure 3: How the risk of death involving COVID-19 varies by religious group for males and females
Hazard ratios of death involving COVID-19 by religious group and sex, England and Wales, 2 March to 15 May 2020
Embed code Embed this interactive Copy
Cox proportional hazards models adjusting for age plus age1. Fully adjusted models also include region, population density, area deprivation, household composition, socio-economic status, Index of Multiple Deprivation (IMD) deciles, highest qualification held, household tenure, multigenerational household flags and occupation indicators (including key workers and exposure to others) in 2011. Fully adjusted models include region indicators, population density, household composition and socio-economic position, highest qualification held, NS-SEC of household person of reference, household tenure, and health status (self-reported health and having a limiting health problem or disability). Office for National Statistics (ONS) figures based on death registrations up to 29 May 2020 that occurred between 2 March and 15 May 2020 that could be linked to the 2011 Census for the coronavirus (COVID-19) rate of death. Risk of death between 2 March and 15 May 2020. Deaths were defined using the International Classification of Diseases, 10th Revision (ICD-10). Deaths involving COVID-19 include those with an underlying cause, or any mention, of ICD-10 codes U07.1 (COVID-19, virus identified) or U07.2 (COVID-19, virus not identified). Error bars not crossing the x-axis at value 1.0 denote a statistically significant difference in relative rates of death. Download this chart .CSV
However, for some religious groups, ethnicity is correlated with religion. That means we cannot be sure whether the observed association between mortality risk involving COVID-19 and religion is because of religion or ethnicity. The impact of ethnicity is explained in Coronavirus (COVID-19) related deaths by ethnic group, England and Wales: 2 March to 15 May 2020. Table 5 shows the breakdown by religious groups by White and non-White ethnic groups regarding deaths involving COVID-19 and populations at risk.
Table 5: Breakdown of deaths and populations of religious groups by a binary breakdown of White and non-White ethnic groups Percentage of deaths involving COVID-19 among White ethnic group Percentage of deaths involving COVID-19 among non-White ethnic groups Percentage identifying as White at the 2011 Census Percentage identifying as non-White at the 2011 Census No religion 94.0 6.0 94.3 5.7 Christian 94.1 5.9 93.0 7.0 Buddhist 26.6 73.4 34.4 65.6 Hindu 1.4 98.6 1.1 98.9 Jewish 95.6 4.4 93.6 6.4 Muslim 7.8 92.2 7.5 92.5 Sikh 1.6 98.4 1.5 98.5 Other religion 66.3 33.7 76.5 23.5 Religion not stated 90.6 9.4 87.4 12.6 View table Download this table .xlsx .csv
Table 5 shows the breakdown by religious groups by White and non-White ethnic groups regarding deaths involving COVID-19 and populations at risk. A full breakdown from the 2011 census can be found in the response to this Freedom of Information request.
We therefore also adjust for whether someone is of White or non-White ethnicity in Figure 4. Adjustment for these factors substantially reduces the risk of death involving COVID-19 relative to those of Christians. More information on how the hazard ratios change when adjusting for different sets of characteristics can be found in the technical appendix. Model diagnostics can be found Model estimates of deaths involving COVID-19 by religious group, England and Wales: 2 March to 15 May 2020. In the fully adjusted model, Jewish males are twice as likely, and females are 1.2 times more likely, to experience a death involving COVID-19 than Christians. Men and women who identify as no religion are around 0.82 and 0.83 times less likely to die from COVID-19, respectively, than Christians.
Figure 4: How the risk of death involving COVID-19 varies by religious group for males and females, adjusted for whether someone is of White or non-White ethnicity
Hazard ratios of death involving COVID-19 by religious group and sex, adjusting for White and non-White ethnic background, England and Wales, 2 March to 15 May 2020
This fully adjusted model (Figure 4), with ethnicity included, demonstrates that a substantial part of the difference in mortality involving COVID-19 between religious groups is explained by the different circumstances in which members of these groups are known to live; for example, living in areas with higher levels of socio-economic deprivation and differences in ethnic makeup. However, for the Jewish group, these factors do not fully explain the difference, suggesting that other causes are still to be identified.
Our adjustment for demographic and socio-economic profile has limitations since the characteristics we use were retrieved from the 2011 Census. Therefore, these may not accurately reflect the study population's circumstances in 2020. While we adjust for some dimensions of health (self-reported health and having a limiting health problem or disability), the information was collected in 2011 and does not distinguish between different types of co-morbidities, which are a likely modifier of the differential risks observed.
Similarly, some religious groups may have a greater propensity to suffer from co-morbidities that are associated with worse outcomes among those infected by COVID-19, which we will take account of in future analyses.
Notes for: Religious group differences in deaths involving COVID-19 adjusted for socio-demographic factors
Migbooty on June 20th, 2020 at 07:38 UTC »
Can't comment on the Jewish death rate but a colleague of mine is Muslim and he has 3 generations of his family living in the same house and in Pakistani and Indian families, this is very common. Perhaps that speeds up the likelihood of infections and deaths in those communities?
AeroOwl19 on June 20th, 2020 at 00:44 UTC »
I think the more interesting correlation is the gender split. Theres clearly a different severity risk for men compared to women
vinbrained on June 19th, 2020 at 23:59 UTC »
No one here has posited a relationship to church? Could this be related to gathering in houses of worship?