Media ads targeting individuals experiencing social anxiety were used for recruitment, and individuals responded by answering online questionnaires on demographics and social anxiety, including the Liebowitz Social Anxiety Scale Self-Report (LSAS-SR)43. All participants were at least 18 years of age, had no neurological disorder, no concurrent psychological treatment and if treated with a psychotropic medication, they agreed to maintain a stable dose at least 3 months before enrollment and during treatment in the current study. All participants also met MRI safety criteria, e.g., not being pregnant and having no ferromagnetic object in the body.
A total of 51 patients with SAD were recruited, but after dropout (n = 2) and incidental findings after initial MRI (n = 3), 46 participants entered treatment. All of them remained for the final assessments. Before treatment and baseline assessments, the patients were interviewed via telephone using the full Mini-International Neuropsychiatric Interview (M.I.N.I.) version 7.0 and the social phobia section of the Structured Clinical Interview for DSM-IV—Axis I Disorders (SCID-I). The patients had to meet the diagnostic criteria for SAD as their principal diagnosis. Patients were excluded if they had a severe ongoing depression (as indexed by scoring > 34 on the self-rated Montgomery Åsberg Depression Rating Scale, MADRS-S)44, current bipolar or psychotic disorders, current alcohol or substance use disorders, or antisocial personality disorder. Other acute illness was not an exclusion criterion.
Four (9%, n = 4/46) patients were on concurrent psychotropic medication, i.e., stable dosage of SSRIs that did not change throughout the study period. Two (4%, n = 2/46) patients had previously used beta blockers in social situations but agreed not to use them during the study period. Seventeen (37%, n = 17/46) had previous experience with some form of psychological treatment but no one had an ongoing therapy. Also, the patients did not change their level of physical exercise during the study, as assessed with a single open-ended question. At the time of recruitment, one patient was on short-term sick leave due to non-psychiatric reasons (and was later not identified as an outlier on any biomarker), all the others were currently employed or students. See Table 1 for a detailed summary of descriptive characteristics. Power calculation based on the main finding in Wolkowitz et al.18 (telomerase activity change correlating with change in depressive symptoms), suggest that the achieved power in this study was above 99%.
Table 1 Demographics, clinical status, concurrent medications, and comorbid conditions in the sample. Full size table
This study used a within-subject design including screening, and two baseline assessments before treatment initiation (pretreatment), and one assessment at posttreatment. Multiple baseline assessments were included to control for standard confounds related to time and measurements, like regression to the mean, repeated testing, and spontaneous remission. Two baseline assessments were separated by 9 weeks, which equals the number of weeks of the current intervention. All 46 patients contributed with complete clinical and biomarker data, and there were no missing data on the primary clinical outcome measure.
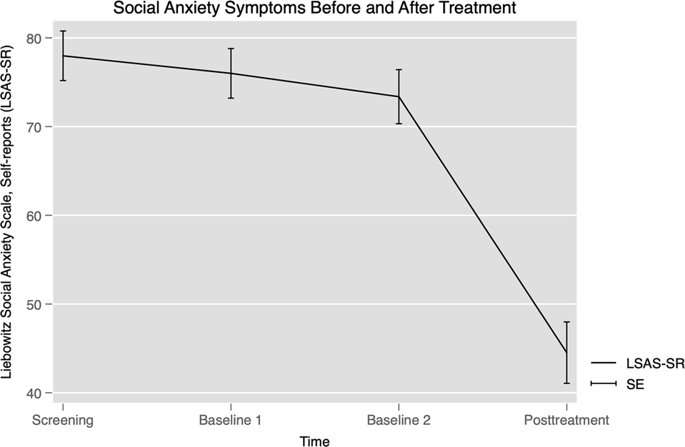
The LSAS-SR is a 24-item self-report questionnaire used internationally to assess treatment-related changes in social anxiety symptoms45. LSAS-SR was the primary outcome and all patients completed assessments at screening, first and second baseline, and posttreatment.
Internet-delivered CBT for SAD has been described extensively elsewhere46,47. Relative to conventional CBT, patients should go through the same behavioral changes, i.e., only the administration format differs. Briefly, the internet-delivered CBT was a guided self-help intervention lasting 9 weeks47. Each week, the patients were provided with a module containing text and homework assignments based on CBT. The content was standardized, i.e., all were provided with the same material, and identical to our previous randomized controlled trials (RCTs), e.g., refs. 47,48. Exposure-based exercises, a main treatment component, were introduced midway, i.e., in the fifth module of the treatment. Patients were in weekly contact with a clinical psychologist providing written feedback and guidance via a secured platform via the Internet. The clinical psychologist provided feedback on the homework assignments, and the patients undertook a weekly test with questions related to CBT and the content of the modules. To control for adherence, the patients had to give 100% correct responses on the multiple-choice questionnaire (with the possibility of redoing the test multiple times). After completion of the homework assignments and the multiple-choice quiz, the next module was made available to the patient.
Seven clinical psychologists were therapists in the current study. Five (n = 71.4%) were licensed clinical psychologists and two (n = 28.6%) were clinical psychology students in their final year and received clinical supervision. At posttreatment, the therapists gave subjective reports on each patient’s compliance to the exposure exercises, and the ratings were “no/minor”, “satisfactory”, or “to a large extent”.
Experienced research nurses collected all blood samples in the morning (from 7:00 a.m. to 11:30 a.m.) after patients had been fasting since 10:00 p.m. the night before. To ensure compliance, all the patients received a mobile phone text message the day before to remind about fasting instructions. The patients were resting for 15 min before the blood was obtained.
Whole blood was obtained in 8 ml BD Vacutainer® CPT™ Mononuclear Cell Preparation Tube—Sodium Citrate (Becton Dickinson). Plasma and mononuclear cells, being lymphocytes and monocytes, were separated within 15 min to 2 h of sampling according to manufacturer’s protocol. Briefly, whole blood was centrifuged for 20 min at 1500 g, whereafter plasma and the mononuclear cell layer were separated and centrifuged again for 15 min at 300 g with phosphate-buffered saline added to the cells for washing. The plasma was immediately frozen at –80 °C. Approximately, half of the pelleted cells were lysed by incubation with 120 µl CHAPS (Merck Millipore, including 0.15 units/µl RiboLock [LifeTechnologies, Thermo Fisher Scientific]) on wet ice for 30 min and three short vortexes, thereafter the lysate was stored at –80 °C.
Approximately, half of the pelleted cells were stored at –80 °C until DNA extraction. Genomic DNA was extracted using DNeasy® Blood & Tissue Kit (Qiagene), with a modified protocol to reduce DNA shearing. Briefly, cell lysis was done at 37 °C for 3 h, vortex was avoided, and centrifugations were performed at 6000 g49. DNA concentration was quantified with NanoDrop ND-1000 Spectrophotometer (Nano-Drop Technologies Inc., Wilmington, DE, USA).
Differential leukocyte counts were determined in whole blood collected in ethylenediaminetetraacetic acid (EDTA) tubes by the University Hospital of Umeå.
Telomerase activity was assayed by modified real-time telomeric repeat amplification protocol50. Samples, controls, and standard curve dilutions were run in triplicate, and standard curve and controls were present on all plates. All samples from each patient were run on the same plate. Efficiency was 95–101%. The mean of the correlation coefficients of the standard curves were all above 0.98. The coefficients of variation (CV) of intra-assay Ct values for the standard dilutions of the four plates was 1.0% and inter-assay was 0.47%. The detection success rate was 100%, and all samples were run in the same batch. See also Supplementary Material.
GPx activity was determined using BioVision Glutathione Peroxidase Activity Colorimetric Assay Kit (Catalog#K726-100) according to the protocol, where the GPx activity was calculated using an NADPH standard curve. The correlation coefficients of the standard curves were all above 0.99. The inter-plate CV of GPx activity was 6.3% and the within-plate CV was 4.4% calculated from positive control run in nine 96-well plates. The assay success rate was 100% (n = 46 at each timepoint), and all samples were run in the same batch. See also Supplementary Material.
Relative telomere length was determined using real-time quantitative PCR according to Cawthon et al.’s protocol51, where the relative telomere to single copy gene (T/S) ratios was determined using a standard curve. In brief, each DNA sample (10 ng) was assessed for the telomere and the single-copy gene (hemoglobin-b, HBB) in triplicate within the same 384-well plate, amplified by using Platinum® SYBR® Green and 0.5 µM of each primer in 10 µl total reaction volume. The correlation coefficients of the standard curves were above 0.99 for each primer set and 384 plate. The inter-plate CV of T/S ratio was 6.3% calculated from a patient sample run in four 384-well plates. The detection success rate was 100%. Samples from all three timepoints per individual were assayed in the same 384-well plate. See also Supplementary Material.
There is evidence that smoking, sex, and body mass index (BMI) are linked to leukocyte telomere length, i.e., smokers52, males53, and high BMI54 are associated with shorter telomeres. Changes in telomerase activity are associated with antidepressant response18. Also, in a large study duration of depressive disorder was inversely associated with telomere length55. In the current study, we were interested in the psychological treatment response in relation to biomarkers, and thus, smoking, BMI, concurrent SSRIs, and duration of illness were considered possible confounders. For calculations of pre–post change in telomerase and telomere length showing statistical significance, change in the proportion of lymphocytes to monocytes was added as a nuisance variable56.
Demographic, clinical, and biomarker statistics were evaluated using the STATA Statistical Software, v. 15.0 (STATA Corporation, College Station, TX, USA).
Generalized Estimating Equations (GEE) with exchangeable correlation structure were used to evaluate panel data on treatment effects across time. Linear regression models were used to assess associations between biomarkers and clinical outcome. The linear regression models including biomarkers and symptom scores were checked for outliers using measures of influence (Cook’s D)57, discrepancy (studentized residuals), and Hosmer–Lemeshow leverage. Individual values with both high influence (Cook’s D > 4/46 = 0.09) and either high residuals (±3) or leverage (>2/46 = 0.04) were determined to be outliers. One patient’s baseline GPx, and two patients’ baseline telomerase were outliers. Three patients’ telomerase change, two patients’ GPx change, and two patients’ change in telomere length were determined to be outliers and excluded from further linear regression. To account for normality violations in biomarkers, nonparametric bootstrapping (×1000) was used to estimate standard errors (Bootstrapped Standard Errors) in the GEE’s and linear regression models.
Within-group effect sizes (Cohen’s d) were based on observed values and calculated by dividing the mean difference with respective standard deviations and correction for the correlation between timepoints. Pre–post change on LSAS-SR was determined by calculating each patient’s change score from pretreatment (mean of the screening, the first and second baseline assessment) to posttreatment [posttreatment – (mean baseline)]. Similarly, the change scores are reported for biomarkers. BMI, sex, duration of SAD, smoking, and concurrent SSRI-treatment were added as covariates in multiple regressions, including the respective biomarker.
vogone on December 27th, 2019 at 10:06 UTC »
Just a reminder to everyone: This was a rather small study with 46 participants.
PM_ME_YOUR_LAWNCHAIR on December 27th, 2019 at 07:54 UTC »
Interesting...
Pr0t0lith on December 27th, 2019 at 07:19 UTC »
This is no real surprise considering how stressful many psychiatric disorders seem to be. It's well understood that living with a high level of stress shortens lifespan considerably.
It is interesting that a mechanism for accelerated aging is presented.