Twenty-nine non-caffeine consumers (<30 mg caffeine/day30) and thirty caffeine consumers (≥150 mg/day40) aged 18–40 participated in Phase I of the study. Twenty-five of the caffeine consumers in Phase I participated in Phase II of the study. Participants were excluded if they displayed any contraindications to exercise (as assessed by the Physical Activity Readiness Questionnaire; PAR-Q), reported cognitive difficulties, reported taking of medication for depression or anxiety, or were pregnant. Prior to participation, each participant read a letter of information outlining all study procedures, as well as potential risks and benefits associated with participation, which was approved by the Western University Research Ethics Board. All study procedures were carried out in accordance with the revised version of the Helsinki Declaration (2013). Informed consent was obtained from all study participants.
Phase I utilized a randomized counterbalanced crossover design such that each participant was randomly assigned treatment order (i.e., caffeine administration followed by exercise or exercise followed by caffeine administration) but completed both treatments irrespective of being non-caffeine and caffeine consumers (Fig. 5). Phase II involved only caffeine consumers and utilized a randomized design such that each participant was randomly assigned to receiving either caffeine administration or exercise following a 12-hour caffeine deprivation period (Fig. 5). Randomization was completed using a computer-generated numbers table.
Figure 5 Schematic representation of study protocol. Full size image
Giles and colleagues38 detected a change in WM accuracy (composite score of hit rate and false alarm rate) between placebo and caffeine administration (Cohen’s d = 0.418). Fagan, Guirguis, Smith, Sui, Rollo, and Prapavessis, unpublished detected a change in WM accuracy (% errors) between baseline and aerobic exercise (Cohen’s d = 0.511). Based on the above findings, to be adequately powered to detect differences from baseline, caffeine, and aerobic exercise, a conservative approach of using a small-to-moderate effect size f = 0.20, power = 0.80, and alpha = 0.05, generated a sample size of 28 individuals23,43.
In developing the Caffeine Withdrawal Symptom Questionnaire (CWSQ), Juliano and colleagues44 detected a 2.69-point reduction in withdrawal symptoms (Cohen’s d = 0.866) when caffeine was administered following a 16-hour caffeine deprivation period. Based on the above findings, to be adequately powered to detect the effects of caffeine administration following an overnight deprivation period, an approach of using the effect size of d = 0.866, power = 0.80, and alpha = 0.05, generated a sample size of 13 individuals23,43.
Age, sex, weight (kg), and education level were collected (Table 1).
Acute and chronic caffeine history (i.e., time of last caffeine consumption, amount of years regularly consuming caffeine, preferred type of caffeine administration) was assessed. Drug and alcohol consumption in the past 18 hours were also assessed (Table 1).
The Physical Activity Readiness Questionnaire (PAR-Q)45 was utilized to assess ability to participate in physical activity safely. The PAR-Q is appropriate to administer to individuals aged 15–69 years45.
The Short Questionnaire to Assess Health-enhancing Physical Activity (SQUASH)46 was administered to assess the frequency, duration, and perceived effort of physical activity during an average week in four domains: commuting (e.g. walking to school), leisure time (e.g. sports), household (e.g. washing dishes), and work/school (e.g. walking and standing between working at a desk)46. Frequency and duration are fillable options, such that the participant is able to indicate the number of days per week, as well as the amount of hours and minutes they partake in each activity, while perceived effort has three possible options: slow/light, moderate, and fast/intense.
The Caffeine Consumption Questionnaire Revised (CCQ-R)47 was administered to assess the consumption of caffeine-containing products (i.e., beverages, foods, and drugs) during an average week. The CCQ-R provides images of caffeine containing products to aid in the estimation of the serving size of products consumed. CCQ-R responses were converted to caffeine intake in milligrams/week using the reference values in Harland40.
Working memory (WM) was assessed through the n-back task. The n-back task has been widely used in the cognition literature to gauge WM, as it requires both short-term recognition of and operation on stimuli48,49. The n-back task consists of a series of stimuli that are presented rapidly on a screen, with the participant deciding whether the target stimuli matches the stimuli ‘n’ items back50. Participants would complete each load (0-back, 1-back, 2-back, and 3-back) three times in a randomized order. The 3-back load is the most cognitively demanding and has been shown to be most sensitive to drug effects51.
The Caffeine Withdrawal Symptom Questionnaire (CWSQ)44 was utilized to assess the type and severity of caffeine withdrawal symptoms experienced by the caffeine consumers. The CWSQ uses twenty-three items which focus on seven symptom clusters: (1) fatigue/drowsiness, (2) low alertness/difficulty concentrating, (3) mood disturbances, (4) low sociability/motivation to work, (5) nausea/upset stomach, (6) flu-like feelings, and (7) headache. The CWSQ also includes nine additional items for consideration, four of which have not yet been empirically validated. Severity of each symptom is assessed on a five-point scale ranging from 0 (not at all) to 4 (extremely). A higher score reflects greater number of symptoms and symptom severity.
The exercise intervention consisted of a single bout of moderate intensity aerobic exercise completed on a Woodway PPS treadmill (Woodway, Waukesh, WI). The intervention consisted of a 2.5 minute warm-up walk, 15 minutes walking at a moderate intensity, and a 2.5 minute cool-down walk. Moderate intensity exercise was defined as 40 to 60% of Heart Rate Reserve (HRR)52,53. The researcher controlled the speed and incline of the treadmill to ensure the participant exercised within their moderate intensity HRR range.
The caffeine administration intervention consisted of oral ingestion of powdered caffeine. Each participant ingested 1.2 mg/kg (body weight) of powdered caffeine (Sigma–Aldrich Foundation, St Louis, MO) dissolved in 100 mL of water39. The participant then waited in a seated position for 20 minutes to permit caffeine absorption53.
Participants were initially screened for eligibility via email or an in-person meeting. For those eligible, a first session was scheduled at the Exercise and Health Psychology Lab. The first session began with administration of the PAR-Q. If a participant indicated yes to any of the seven items on the PAR-Q, they were deemed not able to participate in physical activity and were thus excluded from the study. Upon completion of the PAR-Q, participants were given the demographic questionnaire, caffeine and drug history questionnaire, SQUASH, CCQ-R, and the CWSQ (caffeine consumers only) to complete. A non-caffeine consumer was defined as an individual who consumes less than 30 mg of caffeine/day26. A caffeine consumer was defined as an individual who consumes equal to or greater than 150 milligrams of caffeine a day, which approximately equates to the amount of caffeine in a cup of brewed coffee40. Blood pressure (BP) was taken in a seated position with an electronic sphygmomanometer (MPOW). Resting heart rate (HR) was taken in a seated position with a heart rate monitor (Polar RS100). Weight was measured using the Health-O-Meter Professional weight scale (Health-O-Meter 500 KL, Boca Ration, FL) to the nearest 0.1 kg. Participants then completed the baseline n-back task (lasting approximately 10 to 15 minutes) on a portable computer in isolation. Participants underwent a practice phase to familiarize themselves with the task. The participant needed to score a minimum of 75% of the trials correctly during the practice phase to proceed to the evaluation. The 75% accuracy threshold was deemed appropriate for mitigating the learning effect on the n-back task in a previous study examining WM in smokers and non-smokers (Fagan, Guirguis, Smith, Sui, Rollo, and Prapavessis, unpublished). Upon completion of the baseline n-back task, participants completed either the aerobic exercise or the caffeine administration. HR and BP were again taken at the end of each intervention followed by the n-back task. In session two, participants underwent the intervention they did not receive on session one. All sessions occurred between 8 a.m. and 5 p.m. and were scheduled at approximately the same time of day (i.e., if the participant came in for their baseline session at 8 a.m. all other sessions occurred at the same time) and were separated by a minimum of 24 hours apart. Regarding caffeine consumption during the assessments in Phase I, caffeine consumers were permitted to consume their regular caffeinated products up to 4 hours prior to their session. For example, if a participant was scheduled for a session at 10 am and they have a single serving of coffee normally every day at 6 a.m. they were permitted to do so. However, if their session was at 10 a.m. and they normally have their single serving of coffee between 7 a.m. and 10 a.m. they were not permitted to do so. This strategy mitigates the caffeine consumers from being partially caffeine-withdrawn before testing8.
Caffeine consumers underwent one additional session (Phase II), which required an overnight (12- hour) caffeine deprivation period prior to arrival (i.e., the participant stopped the consumption of any caffeinated products at 8 p.m. and had to come into the lab at 8 a.m.). Participants were told the researcher would be biologically confirming caffeine abstinence through a saliva swab, when in fact no salivary caffeine assays were conducted. This was simply a strategy to increase caffeine deprivation compliance54. Participants’ BP and HR were taken in a seated position upon arrival. They then completed the CWSQ and the n-back task to assess caffeine-deprived performance. Upon completion of the n-back task, participants were randomized into receiving either the exercise session or caffeine administration session. At the end of either session, the CWSQ and n-back were administered again. At the end of the experimental protocols, participants’ email addresses were entered into a draw to win a twenty-five-dollar gift card.
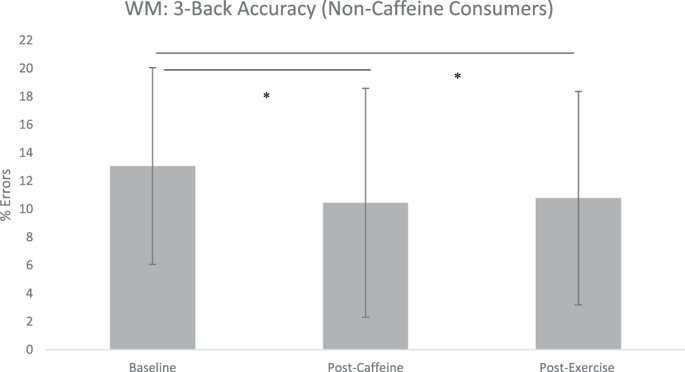
Repeated measures ANOVAs were conducted across baseline, caffeine, and exercise for both accuracy (% errors) and reaction time (RT) in milliseconds (ms) for non-caffeine and caffeine consumers on the n-back task. Analyses focused on the 3-back load. Descriptive data for two, one, and zero-back load can be found under Supplementary Information.
For the caffeine consumers assigned to the caffeine session, a repeated measures ANOVA was conducted across baseline (non-caffeine deprived), caffeine deprived (following 12-hour deprivation), and post-caffeine administration on caffeine withdrawal symptom scores. A repeated measures ANOVA was also conducted across baseline (non-caffeine deprived), caffeine deprived (following 12-hour deprivation), and post-caffeine administration on accuracy and RT on the n-back task. For the caffeine consumers assigned to the exercise session, identical analyses as listed above were conducted. Analyses focused on the 3-back load. Descriptive data for the two, one, and zero-back load can be found under Supplementary Information.
For both phases, all data were assessed for normality (Shapiro-Wilks) and following significant repeated measures ANOVAs, Bonferroni-corrected post-hoc t-tests were conducted. The level of significance was accepted at p ≤ 0.05 for all tests. Effect sizes (Cohen’s d, η2) accompany all reported findings. All bars in figures represent standard deviation (SD). Data were analyzed using IBM SPSS Statistics (Version 23).
pOsEiDoNtRiPlEOg on February 15th, 2020 at 01:29 UTC »
But I can drink coffee while sitting down
444cml on February 15th, 2020 at 01:25 UTC »
I want to note that this study did not demonstrate that
This study demonstrated that, exercise produces comparable cognitive enhancement in a specific cognitive task, through mechanisms that have yet to be elucidated.
I have no doubt that these are overlapping pathways, but your title is as erroneous as saying “based on the fMRI heroin and an orgasm have the same effect on the brain”.
In this study, they don’t try to demonstrate how it acts on the brain, because it’s not what they’re claiming or addressing.
CrnlButtcheeks on February 15th, 2020 at 00:28 UTC »
Wait, is coffee good for memory?